The report reveals the well known and painful truth again for the most powerful and wealthy country in the world…
Mirror, Mirror 2024: An International Comparison of Health Systems | Commonwealth Fund
Cardiology for trainees in cardiology and medicine and any medical professional interested in cardiology. This website has recently been started and is in development. Maintained by Dr Debjit Chatterjee, consultant cardiologist, Medway Maritime Hospital, Kent , UK
The report reveals the well known and painful truth again for the most powerful and wealthy country in the world…
Mirror, Mirror 2024: An International Comparison of Health Systems | Commonwealth Fund
Two articles have been published recently as ‘letters to the editor’ in Heart Rhythm online, about the effect of the newly released iPhone 12 on the function of cardiac implantable electronic devices (CIED), if it is held close to a device. In one article, Greenberg et al.¹ first reported inhibition of tachycardia therapy of a Medtronic implantable cardioverter-defibrillator (ICD) when iPhone 12 was kept close to the device. In the second article, Patterson et al.² compared the effect of iPhone 12 and iPhone XS on CIED of different types and models from different manufactures. The authors of these articles have now conclusively documented that the newly released iPhone 12 can interfere with the function of CIED significantly. iPhone 12 temporarily but consistently inhibited detection of tachyarrhythmia, and hence delivery of appropriate therapy in some models of ICD/cardiac resynchronisation therapy defibrillator. In case of pacemakers, one model (Assurity DR, Abbott) went into asynchronous mode when iPhone 12 was held close to the device. This has caused a huge stir among the cardiologists, common people, and patients with CIED. The overwhelming question now is whether this is going to be a significant public health issue
EP Europace, Volume 24, Issue 2, February 2022, Pages 179–180, https://doi.org/10.1093/europace/euab159
A 35-year-old woman was admitted with atypical chest pain. Her electrocardiogram was normal. There was no rise in serum troponin level. Echocardiogram showed a structurally normal heart with preserved left ventricular systolic function. Her serum cholesterol was very high (total cholesterol of 7.7 mmol/L with LDL of 5.3 mmol/L) but there was no other conventional risk factor for coronary artery disease. In view of ongoing chest pain and high cholesterol, a coronary angiogram was done to rule out coronary artery disease (Figures 1 and 2; Supplementary material online, Videos S1 and S2). Answer: 3. Anomalous origin of left coronary artery from right sinus of Valsalva with retro-aortic course. Explanation Origin of the left main coronary artery (LMCA) from the right sinus of Valsalva is a rare congenital anomaly with an estimated incidence of 0.04%. It has been associated with sudden cardiac death in young persons. Identification of the course of the LMCA after its origin is important to stratify the risk of sudden death. A computed tomography coronary angiogram (CTCA) will identify the course of the LMCA after its origin but in 1985 Ishikawa et al. 1 described a method to determine the course of the LMCA by conventional invasive Figure 2 Left anterior oblique view. Figure 1 Right anterior oblique view.
European Heart Journal. Acute Cardiovascular Care, Volume 11, Issue 5, May 2022, Pages e2–e3, https://doi.org/10.1093/ehjacc/zuac030
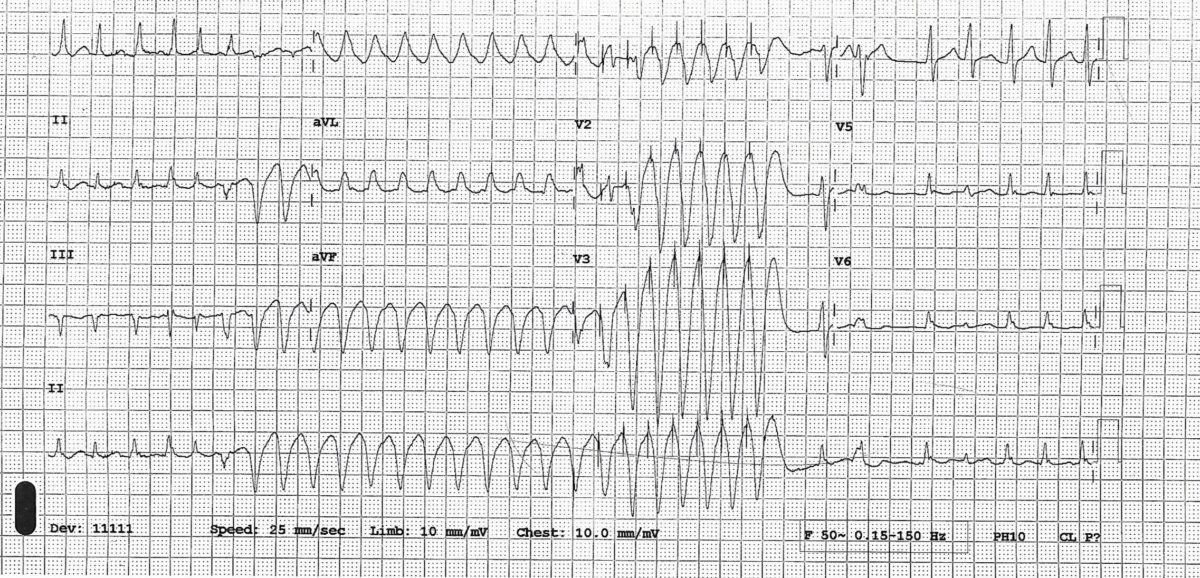
This is an interesting case of wide complex tachycardia in a patient on flecainide for paroxysmal atrial fibrillation. Diagnostic possibilities were discussed, actual diagnosis revealed, and explanation provided.
July 2021Br J Cardiol 2021;28:119–20doi:10.5837/bjc.2021.034
A 71-year-old woman presented to the emergency department (ED) with weakness, dizziness and some episodes of cardiac sounding chest pain for few days. There was no history of diabetes or hypertension and she was a non-smoker.
She saw a cardiologist for dizziness about a year ago. Her ECG showed frequent ventricular ectopics and echocardiogram showed structurally normal heart with preserved LV function and hence she was reassured cardiac wise at that stage. Her dizziness was subsequently thought to be vertigo.
This time she thought her dizziness to be exacerbation of her usual vertigo but episodes of chest pain made her seek medical advice. She was known to have ulcerative colitis and was on mesalazine. On presentation to ED , her hs troponin was 541 (normal < 14). ECG showed T wave inversion in V1-V4.
ECG-

In view of chest pain, increased troponin and ECG changes she was treated as acute coronary syndrome (NSTEMI) and had a coronary angiogram done which showed normal coronary arteries. An echocardiogram showed dyskinesia of the mid and apical part of the LV ventricle with hypercontractile basal segment.
This echo feature is typical of something called Takotsubo cardiomyopathy (because it resembles an octopus pot) or apical ballooning syndrome. See video and still images
This condition was first described in 1990.This happens predominantly in post-menopausal women after severe mental or physical stress and hence is also called broken heart syndrome. There was no obvious trigger in our case. In an international registry of Takotsubo cardiomyopathy patients of 1758 patients 28.5% had no preceding trigger. (1)
The first video shows echocardiogram on this presentation
The second video is echo after 3 weeks
Compare the contraction of mid and apical part of LV in 2 videos
Echo after 3 weeks
Reference:
1. Templin C, Ghadri JR, Dikeman J et al. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. NEJM 2015;373(10):929-38.
2. Yoshihiro J. Akashi, David S. Goldstein, Giuseppe Barbaro and Takashi Ueyama Takotsubo Cardiomyopathy : A New Form of Acute, Reversible Heart Failure. Circulation. December 16/23, 2008,Volume 118, Issue 25
A 49-yr-old woman presented to her general practitioner (GP) with shortness of breath on exertion and mild ankle swelling for few weeks. She was a smoker and initial impression was that she probably suffered from smoking induced chronic obstructive pulmonary disease. Her BNP was slightly raised at 156 pg/ml and hence her GP requested for an open access echocardiogram (TTE) which showed a mass in left atrium. A transoesophageal echocardiogram (TOE) was arranged for further evaluation and it showed the following-
As you can see in transoesophageal echocardiogram, there was a mass in left atrium attached to interatrial septum with a stalk and projecting into the left ventricle through the mitral valve causing obstruction in mitral inflow in diastole. This echo appearance is typical of left atrial myxoma.
Obstructive symptoms and signs–dizziness, sob, cough, pulmonary oedema and heart failure due to obstruction to mitral inflow by the tumour
Embolic manifestations — due to tumour embolism to systemic or pulmonary circulation depending on the location of the tumour
Constitutional features– fever, weight loss, fatigue, myalgia, arthralgia, muscle weakness, Raynaud’s syndrome. They are believed to be due to IL-6 released by myxoma tumour cells (2).
References–
A 22-yr-old man presented to emergency department with acute onset sharp pain across his chest with some radiation to neck. Intensity of the pain did not change with respiration though there was some relief on bending forward. On direct questioning he admitted having sore throat for last 2 days. There were no conventional risk factors for coronary artery disease. On examination there was no murmur or rub.
ECG on the day of admission (ECG 1)
Troponin went from 772 to 1955 (normal up to 13.9), WBC 10.2 ( Normal 4- 10) Neutrophil 7.5 ( Normal 2- 7) CRP not requested
Echo on admission showed bright pericardium with some hypokinesia of LV apical segment. Overall LV function was mildly impaired
ECG after 48 hours (ECG 2)
ECG 1

ECG 2

A diagnosis of myopericarditis was made. Chest pain and ECG changes were suggestive of pericarditis and high troponin and echo findings were evidence of myocardial involvement.
He was treated with ibuprofen and colchicine and was discharged with plan for outpatient cardiac MRI and review in clinic. He was asymptomatic at discharge.
Learning points
1. What did ECGs show? (see the ECG explained below)
ECG 1 showed global concave up ST elevation with reciprocal depression in lead aVR and V1, depressed PR segment (measured from baseline TP segment)
Changes evolved into ECG 2 which showed T wave inversion. Inverted T waves could be evolving changes of pericarditis but sometimes they may be manifestations of myocardial involvement.
Though ECG changes of pericarditis are classically described in 4 stages, not every patient goes through all stages and the duration of each stage varies between patients.

2. What are the differential diagnosis of this ECG?
STEMI
• Will normally show convex upwards ST elevation though can be concave up
• ST elevation will conform to some arterial territory (anterior, inferior etc.) rather than global though on the other hand ECG changes in the pericarditis can sometimes be localised
• Reciprocal ST depression in leads other than aVR and V1
Early repolarisation
• ST elevation not global (usually inferolateral)
• No PR depression
•No evolution in ST changes over time
ESC guidelines 2015–

This is a straightforward but exceedingly rare ECG.
A 70-yr-old man presented with an episode of collapse. He was known to have severe LV systolic dysfunction and atrial fibrillation for a while. His coronaries were unobstructed, and his ECG showed-

As you can see ECG shows LBBB with right axis and atrial fibrillation. LBBB and right axis is a rare combination. LBBB is usually associated with normal or left axis. LBBB with right axis usually indicates biventricular enlargement and diffuse conduction system disease.
From a database of 636,000 electrocardiograms a series of only 36 patients with this combination was described. Most subjects had dilated cardiomyopathy with biventricular enlargement. (1)
References
1. Childers R1, Lupovich S, Sochanski M, Konarzewska H. Left bundle branch block and right axis deviation: a report of 36 cases. J Electrocardiol. 2000;33 Suppl:93-102.
A 71-yr-old man was admitted with increased shortness of breath and pedal swelling for few days. He was known to suffer from COPD and this admission was thought to be due to acute infective exacerbation. There was no cardiac history. On admission there was significant tachycardia and ECG (ECG 1 and 2) was done. The rhythm was mentioned as atrial fibrillation in his notes. Echocardiogram showed preserved LV systolic function, dilated right ventricle with moderate tricuspid regurgitation, pulmonary artery pressure could not be measured because of poor echo window and TR could only be visualised in subcostal view.
What is the true rhythm in ECG?
ECG 1

ECG 2

The rhythm is multifocal atrial tachycardia (also called chaotic atrial tachycardia) and not AF.
● There are multiple morphologies of P wave (classically described as at least 3 morphologies). PP intervals are irregular; most P waves are conducted to the ventricles though with varying PR intervals leading to irregular RR intervals creating a general impression of AF
● This rhythm usually occurs in older patients with COPD or congestive heart failure and may eventually develop into atrial fibrillation
● Digoxin and theophylline administration can be causally related
● Management is primarily that of underlying disease. Beta blocker is helpful if tolerated but is usually avoided because of associated obstructive airway disease. Non-dihydropyridine calcium channel blockers (diltiazem, verapamil) and amiodarone may be helpful. There is some evidence that IV magnesium may control the rate or even revert it to sinus rhythm.
 in diastole
in diastole