Author: Debjit Chatterjee
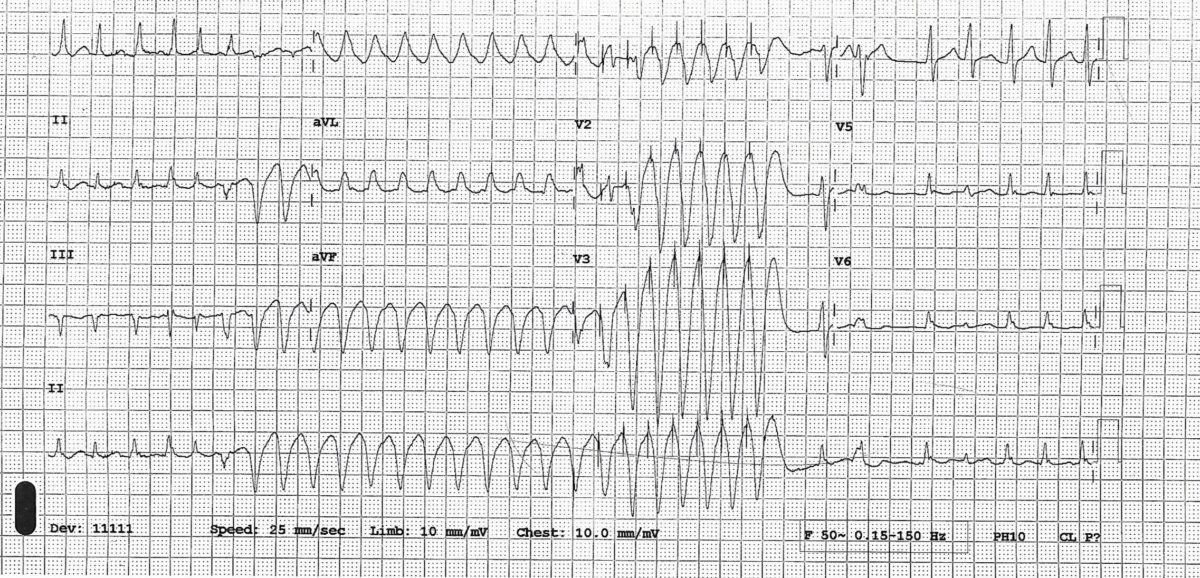
Atrial flutter with 1:1 AV conduction, a case series
Cardiology Journal Watch 9th Feb 2024
Cardiology Journal watch 9th Feb 2024
Debjit Chatterjee
ORBITA2
Dec 2023 NEJM
Among patients with stable angina who were receiving little or no antianginal medication and had objective evidence of ischemia, PCI resulted in a lower angina symptom score ( improvement in angina) than a placebo procedure
– double-blind, randomized, placebo-controlled trial
-300 patients randomised to either PCI or placebo procedure in 1: 1 ratio
– All patients had non-invasive evidence of ischaemia before coronary angiogram
-Follow up for 12 weeks (1)
In an editorial regarding the above study in NELM, the comments are (2)
The ORBITA-2 trial will influence patient care, guidelines, and the design of new trials. one can think now of two evidence-based pathways for the management of stable angina:
-initial medical therapy, and then PCI if the medical therapy fails to relieve symptoms or if the patient develops unacceptable side effects from antianginal medication,
-or PCI without the use of antianginals with the addition of medical therapy if the symptoms continue.
-The pros and cons of both pathways should be discussed with the patient, including the risks of PCI, the chance of stent thrombosis (0.5% per year), and the need for dual antiplatelet therapy with the associated risk of bleeding.
Patients should express a preference, which is important.
Angiographic findings may tilt the decision towards one or other. Implanting a stent in a small branch vessel in a patient who has a high risk of stent thrombosis may be inappropriate
References-
- Rajkumar CA, Foley MJ, Ahmed-Jushuf F et al A Placebo-Controlled Trial of Percutaneous Coronary Intervention for Stable Angina, for the ORBITA-2 Investigators. n engl j med 389;25 nejm.org December 21, 2023
- Changing the Orbit around Percutaneous Coronary Intervention for Stable Angina Harvey D. White, D.Sc. n engl j med 389;25 nejm.org December 21, 2023
ARTESIA
January 11 , 2024 NEJM
Among patients with subclinical atrial fibrillation, apixaban resulted in a lower risk of stroke or systemic embolism than aspirin but a higher risk of major bleeding
Subclinical AF = Any AF detected in Pacemaker or ICD of 6miniutes to 24 hours duration
Total of 4012 patients
Mean CHA2DS2VASc Was 3.9 +_ 1.1
Mean follow up 3.5 +_ 1.8 years
Stroke or systemic embolism occurred in 0.78% per patient year in apixaban group versus 1.24% per patient year P= 0.007
Major bleeding happened in 1.71% per patient year versus 0.94% per patient year in aspirin group P = 0.001. Fatal bleeding occurred in 5 patients in apixaban group versus 8 patients in aspirin group (1)
Compare this results with another similar trial— NOAH-AFNET6 ( published in Sept 2023 in NEJM) in similar group of patients , edoxaban, as compared with placebo, did not provide a benefit with respect to the primary efficacy outcome (Stroke, systemic embolism , cardiovascular death) and was associated with a higher incidence of a composite of death or major bleeding. Analysis of stroke was underpowered because of small number of stroke. (2)
References-
1.Healey JS, Lopes RD, Granger CB et al .Apixaban for Stroke Prevention in Subclinical Atrial Fibrillation. For the ARTESIA Investigators. N Engl J Med 2024; 390:107-117 DOI: 10.1056/NEJMoa2310234
- Kirchhof P, Toennis T, Goette A, et al. Anticoagulation with edoxaban in patients with atrial high-rate episodes. N Engl J Med 2023;389:1167-79.