A 22-yr-old man presented to emergency department with acute onset sharp pain across his chest with some radiation to neck. Intensity of the pain did not change with respiration though there was some relief on bending forward. On direct questioning he admitted having sore throat for last 2 days. There were no conventional risk factors for coronary artery disease. On examination there was no murmur or rub.
ECG on the day of admission (ECG 1)
Troponin went from 772 to 1955 (normal up to 13.9), WBC 10.2 ( Normal 4- 10) Neutrophil 7.5 ( Normal 2- 7) CRP not requested
Echo on admission showed bright pericardium with some hypokinesia of LV apical segment. Overall LV function was mildly impaired
ECG after 48 hours (ECG 2)
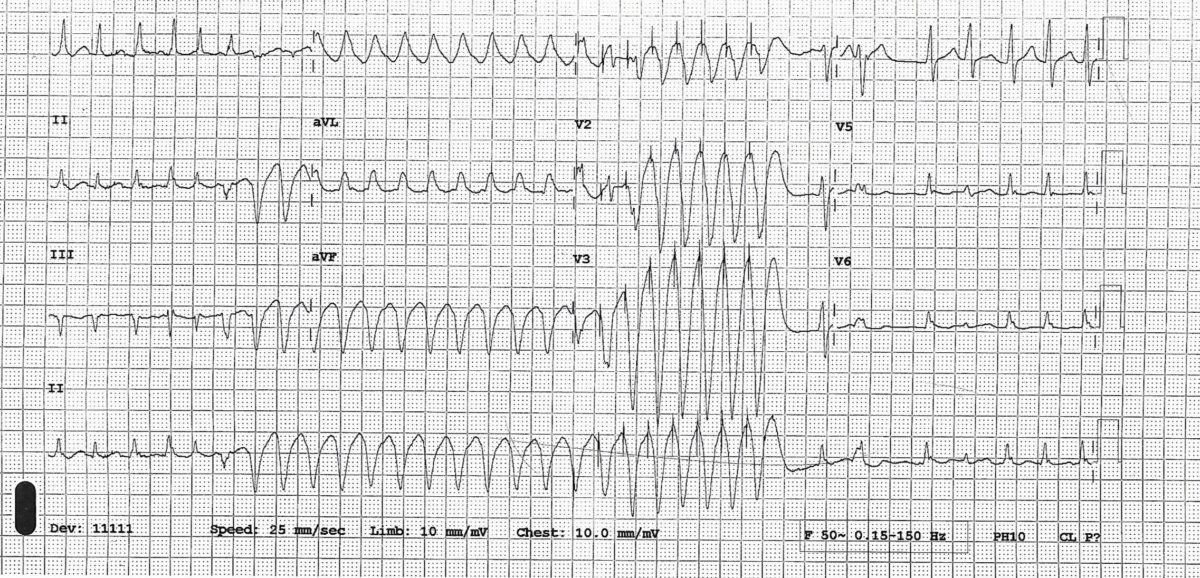
ECG 1

ECG 2

A diagnosis of myopericarditis was made. Chest pain and ECG changes were suggestive of pericarditis and high troponin and echo findings were evidence of myocardial involvement.
He was treated with ibuprofen and colchicine and was discharged with plan for outpatient cardiac MRI and review in clinic. He was asymptomatic at discharge.
Learning points
1. What did ECGs show? (see the ECG explained below)
ECG 1 showed global concave up ST elevation with reciprocal depression in lead aVR and V1, depressed PR segment (measured from baseline TP segment)
Changes evolved into ECG 2 which showed T wave inversion. Inverted T waves could be evolving changes of pericarditis but sometimes they may be manifestations of myocardial involvement.
Though ECG changes of pericarditis are classically described in 4 stages, not every patient goes through all stages and the duration of each stage varies between patients.

2. What are the differential diagnosis of this ECG?
STEMI
• Will normally show convex upwards ST elevation though can be concave up
• ST elevation will conform to some arterial territory (anterior, inferior etc.) rather than global though on the other hand ECG changes in the pericarditis can sometimes be localised
• Reciprocal ST depression in leads other than aVR and V1
Early repolarisation
• ST elevation not global (usually inferolateral)
• No PR depression
•No evolution in ST changes over time
ESC guidelines 2015–
